
Healthcare Risk Management: Best Practices That Actually Work
Why Do So Many Medical Facilities Still Treat Risk as an Afterthought?

Healthcare risk management best practices encompass systematic protocols designed to identify, assess, mitigate, and monitor clinical, operational, financial, and technological threats within medical facilities. These evidence-based frameworks integrate patient safety, regulatory compliance, financial liability reduction, and cybersecurity defense. When properly implemented, they reduce adverse events, contain malpractice costs, safeguard protected health information (PHI), and preserve institutional reputation across increasingly complex care delivery environments.
Have you ever walked into your facility on a Monday morning to discover that a billing error triggered a federal audit, or that a staff member’s workaround on a medication protocol nearly harmed a patient over the weekend? If you manage or oversee a clinic, hospital, or multi-site health network, these scenarios probably feel less hypothetical and more like Tuesday. The financial toll alone is staggering; the human cost is immeasurable. What you need is not another checklist pinned to a breakroom wall. You need a working system that anticipates threats before they become crises and protects both your patients and your organization’s financial future. The information ahead delivers exactly that. It draws on current research, cross-border regulatory realities, and hard-won institutional experience to give you a genuinely actionable framework.
📌 Executive Summary — Key Takeaways
⚡ Critical Financial Facts
- Average healthcare data breach cost: $10.93 million (highest of any industry, 13 consecutive years)
- Average malpractice indemnity payment: over $380,000 per claim; high-risk specialties can reach millions per case
- Average hospital operating margin: just 2.1% — a single major settlement can eliminate an entire year’s surplus
- U.S. healthcare fraud recoveries: over $2.1 billion in 2024 under the False Claims Act
🛠️ Immediate Action Steps
- Implement proactive cybersecurity measures (penetration testing, phishing simulations, incident response plans) — investment of $45,000+ annually can prevent losses of millions
- Adopt communication-and-resolution programs (CRPs) to reduce malpractice claim costs by 36% and claim volume by 44%
- Build a just culture to increase voluntary incident reporting by 45% and decrease repeat adverse events by 22%
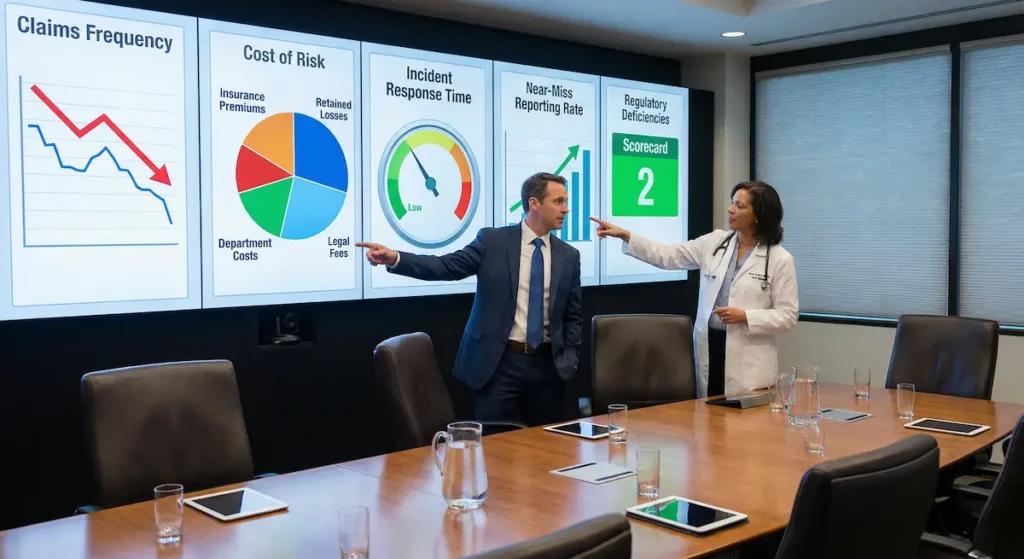
- Track five core KPIs: claims frequency, cost of risk, incident response time, near-miss reporting rate, and regulatory deficiency rates
🚨 Core Risk Warning
- Organizations with mature risk management programs experience 38% lower total cost of risk — those without structured programs face escalating financial exposure across clinical, operational, regulatory, and technological fronts simultaneously
- New HIPAA cybersecurity requirements (multi-factor authentication, 72-hour breach reporting) are pending finalization — early preparation is essential
Source: AHRQ • IBM Security • ASHRM
What Does a Real-World Risk Failure Actually Look Like?
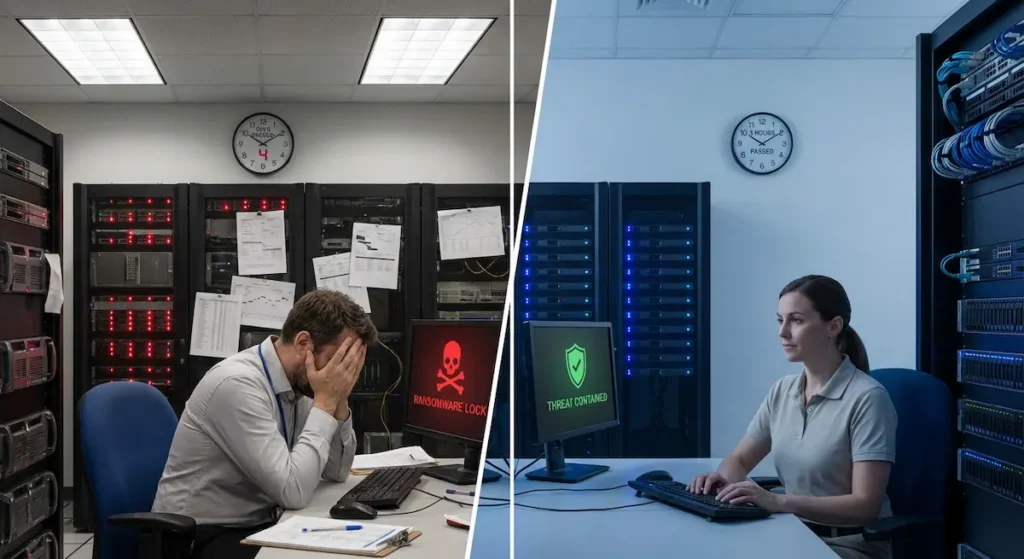
Consider a mid-sized orthopedic surgery center in the American Southeast, circa 2023. The facility had a solid reputation, strong patient satisfaction scores, and healthy revenue. Then a single phishing email compromised its electronic health records (EHR) system. For 11 days, staff reverted to paper charting. Scheduled surgeries were delayed. The ransomware attackers demanded $1.2 million. The center’s cyber liability insurance covered roughly 60% of direct costs, but it could not cover the reputational damage, the patient attrition, or the 14 months of litigation that followed. An internal review later revealed that the facility had never conducted a formal cybersecurity risk assessment, despite handling thousands of patient records containing Social Security numbers, insurance data, and clinical histories.
Now reverse the scenario. Imagine that same facility had invested $45,000 annually in penetration testing, staff phishing simulations, and an incident response plan. The email still arrives. A staff member still clicks it. But the system detects the anomaly within minutes, isolates the affected workstation, and triggers the response protocol. Downtime: 3 hours instead of 11 days. Financial exposure: a fraction. Patient trust: intact. This is the difference between reactive and proactive risk management — and it applies equally to clinical errors, compliance gaps, and financial vulnerabilities.
| Comparison Dimension | Reactive Risk Management | Proactive Risk Management |
|---|---|---|
| Core Philosophy | Respond to events after they occur | Anticipate and prevent events before they occur |
| Primary Data Source | Post-incident reports and claims history | Predictive analytics, near-miss data, and prospective risk assessments |
| Timing of Intervention | After harm has reached the patient or financial loss has occurred | Before harm reaches the patient or financial loss materializes |
| Financial Exposure (Cybersecurity Example) | Average healthcare breach cost: $10.93 million (2023) | Annual proactive investment: $45,000–$150,000 for penetration testing and response planning |
| Downtime After Cyberattack | Days to weeks (average 11 days in case study) | Hours (3 hours in case study with incident response plan) |
| Malpractice Claims Strategy | Traditional “deny and defend” approach | Communication-and-resolution programs (CRPs): 36% lower claim costs, 44% fewer claims |
| Safety Culture Indicator | Low incident reporting; culture of silence or blame | High near-miss reporting; just culture with 45% increase in voluntary reports |
| Patient Safety Model | Incident review committees convened after adverse events | Early warning score systems reducing cardiac arrest rates by up to 30% |
| Total Cost of Risk Impact | Higher total cost of risk; unpredictable financial exposure | 38% lower total cost of risk in mature programs (JHRM, 2022) |
| Board-Level Integration | Risk discussed only after major incidents or litigation | Risk dashboards reviewed regularly; CFO and CMO share accountability |
|
Source: https://www.ahrq.gov/patient-safety/resources/index.html Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services |
||
What Are the 4 Pillars of Comprehensive Healthcare Risk Management?

To build a program that actually works, administrators must address four interdependent domains. Neglecting any single pillar weakens the entire structure. Let us examine each one with the specificity it demands.
| Risk Pillar | Primary Threat | Key Financial Impact | Core Mitigation Strategy | Key Metric |
|---|---|---|---|---|
| Clinical Risk | Preventable adverse events, diagnostic errors, medication errors | Average malpractice indemnity exceeding $380,000 per claim (2023) | Standardized care protocols, SBAR/I-PASS handoffs, root cause analysis | Claims frequency per 1,000 patient encounters |
| Operational Risk | Staffing shortages, supply chain disruption, credentialing gaps | Increased clinical error rates, overtime costs, agency staffing premiums | Workforce planning, supplier diversification, facility maintenance programs | Patient-to-nurse ratios and staff vacancy rates |
| Financial Risk | Malpractice claims, billing fraud, coding errors, regulatory penalties | Over $2.1 billion in U.S. fraud recoveries (2024); average hospital margin just 2.1% | Insurance optimization, internal auditing aligned with OIG Work Plan, CRPs | Cost of risk as percentage of net patient revenue |
| Technological Risk | Ransomware, data breaches, IoMT device vulnerabilities | Average healthcare breach cost $10.93 million (2023) | Network segmentation, encryption, penetration testing, incident response plans | Incident response time and breach detection speed |
|
Source: https://www.ahrq.gov/patient-safety/resources/index.html Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services |
||||
Why Is Clinical Risk the Foundation of Everything Else?
Clinical risk — the possibility that patient care will result in harm, adverse outcomes, or death — sits at the center of every medical facility risk management conversation. A study published in the BMJ Quality & Safety journal in 2023 estimated that preventable adverse events contribute to over 250,000 deaths annually in the United States alone, making medical error the third leading cause of death behind heart disease and cancer. In the United Kingdom, NHS Resolution reported paying £2.7 billion in clinical negligence claims for the fiscal year 2022–2023.
What does effective clinical risk management look like day to day? It starts with standardized care protocols, evidence-based clinical pathways, and real-time monitoring of patient outcomes. It includes structured handoff communication — the “I-PASS” or “SBAR” frameworks — to prevent information loss during shift changes. It requires root cause analysis (RCA) after every sentinel event, not just the ones that attract media attention.
💡 Did You Know?
The “Swiss Cheese Model” developed by James Reason remains one of the most widely referenced frameworks in patient safety. It illustrates that adverse events occur not because of a single failure, but because multiple layers of defense each have a “hole” — and those holes momentarily align. Strengthening any single layer reduces the probability of harm reaching the patient.
https://www.bmj.com/content/320/7237/768
Reason, J. (2000). “Human error: models and management.” BMJ, 320(7237), 768–770.
How Do Operational Risks Quietly Erode a Facility’s Stability?
Operational risk covers a broad spectrum: staffing shortages, supply chain disruptions, facility maintenance failures, credentialing gaps, and vendor management breakdowns. The COVID-19 pandemic exposed how fragile hospital supply chains truly were. Facilities that had not diversified their suppliers for personal protective equipment (PPE), ventilator components, and essential medications faced life-threatening shortages within weeks.
Staffing represents another critical operational risk. The Australian Institute of Health and Welfare (AIHW) reported in 2024 that nursing shortages in rural and remote areas continue to force facilities into dangerous patient-to-nurse ratios. Meanwhile, in the United States, the Bureau of Labor Statistics projects the healthcare sector will need to fill over 2 million new positions by 2031. Understaffing does not merely create burnout; it directly increases clinical error rates, which feeds back into clinical risk and, ultimately, financial liability.
What Makes Financial Risk So Uniquely Dangerous in Healthcare?
Financial risk in healthcare operates on multiple fronts. Malpractice claims represent the most visible threat. According to data from the Physician Insurers Association of America, the average indemnity payment for a malpractice claim exceeded $380,000 in 2023. In high-risk specialties like obstetrics and neurosurgery, that figure can reach several million dollars for a single case. But malpractice is only one dimension.
Billing fraud, whether intentional or resulting from coding errors, triggers audits, clawbacks, and potential exclusion from government payer programs. In 2024, the U.S. Department of Justice recovered over $2.1 billion in healthcare fraud settlements under the False Claims Act. In Australia, the Medicare Benefits Schedule (MBS) Review Taskforce has intensified scrutiny on inappropriate billing patterns, and in the United Kingdom, NHS Counter Fraud Authority investigations recovered £90 million in 2023 alone. These are not abstract numbers. They represent existential threats to facilities operating on thin margins.
📈 Surprising Stat
According to the American Hospital Association, the average hospital operating margin in 2023 was just 2.1%. A single large malpractice settlement or billing fraud penalty can wipe out an entire year’s operating surplus.
https://www.aha.org/costsofcaring
American Hospital Association (AHA) — Costs of Caring Report, 2024
Read also: Corporate Banking Solutions for Healthcare: A Compliance-Focused Guide for Medical Practices
Why Has Technological Risk Become the Fastest-Growing Threat?
Healthcare cybersecurity risk management has moved from the IT department’s concern to the boardroom’s top agenda item. The U.S. Department of Health and Human Services (HHS) reported that healthcare data breaches affecting 500 or more individuals increased by 93% between 2018 and 2023. The average cost of a healthcare data breach reached $10.93 million in 2023, according to IBM’s annual Cost of a Data Breach report — the highest of any industry for the 13th consecutive year.
Connected medical devices — infusion pumps, MRI machines, pacemaker programmers — expand the attack surface dramatically. Many of these devices run outdated operating systems that no longer receive security patches. A compromised insulin pump is not merely a data privacy issue; it is a patient safety emergency. This intersection of technological and clinical risk demands an integrated approach that no single department can manage alone.
How Can Facilities Shift From Reactive to Predictive Patient Safety?

For decades, patient safety protocols relied on incident reporting: something goes wrong, someone fills out a form, a committee reviews it, and recommendations are issued. This reactive model has saved countless lives. But it has a fundamental limitation. It only captures events that have already occurred. Predictive safety models, by contrast, use data analytics, machine learning, and prospective risk assessments to identify dangerous patterns before they produce harm.
Consider the early warning score (EWS) systems now deployed in hospitals across the US, UK, and Australia. These tools aggregate physiological data — heart rate, blood pressure, respiratory rate, oxygen saturation, temperature — into a single composite score. When the score crosses a threshold, the system triggers an escalation response, often before bedside clinicians have recognized the deterioration. A study published in Resuscitation in 2020 found that the National Early Warning Score 2 (NEWS2) reduced cardiac arrest rates in UK hospitals by as much as 30% when properly implemented.
Standardized care pathways represent another proactive strategy. When every clinician follows the same evidence-based protocol for managing sepsis, venous thromboembolism prophylaxis, or surgical site infection prevention, clinical variance decreases. Clinical variance is, at its core, a risk multiplier. Every deviation from an evidence-based standard introduces the possibility of a suboptimal outcome. This does not mean eliminating clinical judgment. It means ensuring that departures from standard care are deliberate, documented, and defensible.
🔒 Key Insight
The distinction between a “near-miss” and an “adverse event” is often pure chance — not a reflection of risk severity. Facilities that treat near-misses with the same analytical rigor as actual adverse events consistently outperform those that do not.
https://psnet.ahrq.gov/primer/close-calls-near-misses
AHRQ Patient Safety Network (PSNet) — Close Calls (Near Misses) Primer
How Should Medical Facilities Approach Financial Risk Mitigation?

Financial risk in healthcare demands a two-pronged approach. The first prong addresses malpractice exposure. The second addresses revenue cycle integrity. Both require sustained attention from clinical and administrative leadership working together — not in separate silos.
Malpractice insurance optimization begins with understanding your facility’s specific risk profile. A rural primary care clinic does not carry the same exposure as a Level I trauma center performing complex neurosurgical procedures. Yet many facilities accept renewal quotes from their existing insurer without conducting a comparative market analysis. Insurance brokers specializing in medical professional liability can identify coverage gaps, negotiate better terms, and recommend loss-sensitive programs (such as experience-rated or retrospectively-rated policies) that reward facilities with strong safety records through reduced premiums.
Claims management matters just as much as coverage selection. When an adverse event occurs, the speed and quality of the initial response often determine the ultimate financial outcome. Effective risk management strategies for hospitals include immediate event documentation, preservation of relevant records, early engagement of defense counsel, and transparent communication with the affected patient and family. A study published in Health Affairs in 2019 demonstrated that communication-and-resolution programs (CRPs), where facilities proactively disclose errors and offer fair compensation, reduced average malpractice claim costs by 36% and total claims volume by 44% compared to traditional “deny and defend” approaches.
Revenue cycle compliance is equally significant. In the United States, the Office of Inspector General (OIG) publishes an annual Work Plan identifying its enforcement priorities. Facilities that align their internal auditing programs with OIG priorities — upcoding, unbundling, duplicate billing, medical necessity documentation — position themselves to identify and correct problems before external auditors arrive. In Australia, the Department of Health’s compliance program for the MBS follows similar principles. The message across all three jurisdictions is identical: self-audit aggressively, correct errors promptly, and document your compliance efforts meticulously.
⚖️ Malpractice Strategy Comparison
Compare “Deny & Defend” vs. Communication & Resolution Programs (CRP).
Read also: The Complete Guide to Personal Financial Management: Your Guide from Zero to Financial Stability
Are You Truly Prepared for Regulatory Scrutiny Across Borders?
Regulatory compliance in healthcare is not static. Regulations change, enforcement priorities shift, and penalties escalate. What distinguished compliant facilities from vulnerable ones is not the absence of risk — it is the presence of systems designed to detect and adapt to regulatory change in real time.
In the United States, the regulatory landscape includes the Health Insurance Portability and Accountability Act (HIPAA) for data privacy, the Occupational Safety and Health Administration (OSHA) for workplace safety, the Emergency Medical Treatment and Labor Act (EMTALA) for emergency department obligations, and the Stark Law and Anti-Kickback Statute for physician self-referral and financial arrangements. Each carries its own enforcement mechanisms and penalty structures. HIPAA violations alone can result in fines of up to $2.1 million per violation category per year, as adjusted for inflation under the HITECH Act.
In the United Kingdom, the Care Quality Commission (CQC) serves as the independent regulator for health and social care. Its inspection framework evaluates services across five domains: safety, effectiveness, caring, responsiveness, and leadership. Facilities rated as “Inadequate” face conditions, restrictions, or outright closure. Furthermore, the General Data Protection Regulation (GDPR), retained in UK law post-Brexit, imposes data protection obligations with fines of up to £17.5 million or 4% of annual global turnover, whichever is higher.
Australia’s regulatory framework includes the Australian Commission on Safety and Quality in Health Care (ACSQHC), which sets the National Safety and Quality Health Service (NSQHS) Standards. Accreditation against these standards is mandatory for all hospitals and day procedure services. The Australian Prudential Regulation Authority (APRA) and the Office of the Australian Information Commissioner (OAIC) add financial and data privacy layers respectively. The OAIC can impose penalties of up to AUD $50 million for serious or repeated privacy breaches under the Privacy Act 1988, as amended in 2022.
| Compliance Dimension | United States | United Kingdom | Australia |
|---|---|---|---|
| Data Privacy Law | HIPAA / HITECH Act | UK GDPR (retained EU regulation) | Privacy Act 1988 (amended 2022) |
| Maximum Data Privacy Penalty | Up to $2.1 million per violation category per year | Up to GBP 17.5 million or 4% of annual global turnover | Up to AUD 50 million for serious or repeated breaches |
| Quality & Safety Regulator | CMS / The Joint Commission / State Health Departments | Care Quality Commission (CQC) | Australian Commission on Safety and Quality in Health Care (ACSQHC) |
| Accreditation Standards | CMS Conditions of Participation; Joint Commission standards | CQC Fundamental Standards (5 domains: Safe, Effective, Caring, Responsive, Well-led) | National Safety and Quality Health Service (NSQHS) Standards, 2nd edition |
| Fraud Enforcement Body | U.S. Department of Justice (DOJ) / OIG | NHS Counter Fraud Authority | Department of Health / Medicare Benefits Schedule (MBS) Review Taskforce |
| Annual Fraud Recoveries (Latest Available) | Over $2.1 billion (2024, False Claims Act) | GBP 90 million (2023) | Subject to ongoing MBS compliance audits (figures vary by year) |
| Workplace Safety Regulator | OSHA (Occupational Safety and Health Administration) | Health and Safety Executive (HSE) | Safe Work Australia / State-level regulators |
| Emergency Care Obligation | EMTALA (Emergency Medical Treatment and Labor Act) | NHS Constitution patient rights; A&E 4-hour standard | National Emergency Access Target (NEAT) benchmarks |
|
Source: https://www.who.int/health-topics/health-systems-governance World Health Organization (WHO) — Health Systems Governance and Financing |
|||
⚠️ Regulatory Alert
In 2024, the U.S. Department of Health and Human Services proposed new cybersecurity requirements for HIPAA-covered entities, including mandatory multi-factor authentication, network segmentation, and 72-hour incident reporting. Facilities that delay preparation will face significant compliance costs once these rules are finalized.
https://www.hhs.gov/hipaa/for-professionals/security/hipaa-security-rule-nprm/index.html
U.S. Department of Health and Human Services (HHS) — HIPAA Security Rule NPRM, 2024
Read also: Understanding the Dodd-Frank Act Requirements for Banks in 2026
How do top-performing facilities stay ahead? They designate a compliance officer or committee with direct reporting authority to the board. They subscribe to regulatory update services from organizations like the Healthcare Compliance Association (HCCA) or the Australasian Association for Quality in Health Care (AAQHC). They conduct mock surveys and internal audits at least annually. Most critically, they view compliance not as a cost center but as a risk management investment.
What Makes Healthcare Facilities Such Attractive Targets for Cyberattacks?
The answer is painfully straightforward. Healthcare organizations hold extraordinarily valuable data — complete patient identities including names, dates of birth, Social Security or Medicare numbers, insurance details, and clinical histories — and they often protect it with inadequate defenses. A stolen credit card number sells for $1 to $2 on dark web markets. A stolen health record sells for $250 to $1,000. The economic incentive for attackers is overwhelming.
Ransomware attacks on hospitals have escalated sharply. The Ponemon Institute’s 2023 report on healthcare cybersecurity found that 88% of surveyed healthcare organizations experienced at least one cyberattack in the preceding 12 months. Among those, 57% reported that the attack adversely affected patient care, including longer lengths of stay, delayed procedures, and increased mortality rates.
Securing EHRs requires a layered defense strategy. Network segmentation isolates clinical systems from administrative ones, limiting lateral movement by attackers. Encryption at rest and in transit protects data even if it is intercepted. Access controls based on the principle of least privilege ensure that staff members can only view the patient data necessary for their roles. Regular vulnerability scanning and penetration testing identify weaknesses before attackers exploit them.
| Year | Average Cost per Healthcare Breach (USD Millions) | Healthcare Rank Among All Industries | Breach Volume Change (Year-over-Year) |
|---|---|---|---|
| 2018 | $6.45 | #1 (Highest) | Baseline Year |
| 2019 | $6.45 | #1 (Highest) | +0% |
| 2020 | $7.13 | #1 (Highest) | +10.5% |
| 2021 | $9.23 | #1 (Highest) | +29.5% |
| 2022 | $10.10 | #1 (Highest) | +9.4% |
| 2023 | $10.93 | #1 (Highest — 13th consecutive year) | +8.2% |
|
Source: https://www.ibm.com/reports/data-breach IBM Security — Cost of a Data Breach Report (2018–2023) |
|||
Connected medical devices (the Internet of Medical Things, or IoMT) present unique challenges. Many legacy devices cannot be updated or patched. For these, compensating controls — network isolation, traffic monitoring, and device inventory management — become essential. The U.S. Food and Drug Administration (FDA) issued updated guidance in 2023 requiring manufacturers of new medical devices to submit cybersecurity plans as part of the premarket approval process. This is a welcome development, but it does not address the millions of devices already in service.
The hidden costs of a data breach extend far beyond the immediate ransom payment or regulatory fine. Legal defense costs, forensic investigation fees, patient notification expenses, credit monitoring services, operational downtime, and long-term reputational damage compound over months and years. A 2023 analysis by Comparitech found that publicly traded healthcare companies experienced an average stock price decline of 7.5% in the 6 months following a major data breach disclosure.
💡 Did You Know?
The first known ransomware attack on a hospital occurred in 2016, when Hollywood Presbyterian Medical Center in Los Angeles paid $17,000 in Bitcoin to regain access to its systems. By 2024, the average ransomware demand against healthcare organizations had reached $1.5 million — an 88-fold increase in less than a decade.
https://ocrportal.hhs.gov/ocr/breach/breach_report.jsf
U.S. Department of Health and Human Services, Office for Civil Rights — Breach Portal
🔒 Cyber Breach Impact Estimator
Estimate financial exposure based on record count and downtime.
Read also: How to Secure Your Crypto Account: The Complete 2FA Setup Guide
Why Is a “Just Culture” the Most Underrated Risk Management Tool?

Every clinical risk management framework depends on data. Incident reports, near-miss disclosures, safety observations, and staff concerns form the raw material from which risk patterns emerge. But here is the fundamental problem: if staff members fear punishment for reporting errors or near-misses, they will not report them. The data pipeline dries up. Hazards remain invisible until they produce catastrophic harm.
A “just culture” framework, first articulated by David Marx and widely adopted following James Reason’s work on human error, distinguishes between three types of behavior. Human error (a slip, lapse, or mistake made by a competent professional acting in good faith) warrants consolation and system redesign. At-risk behavior (a conscious deviation from safe practice where the individual did not appreciate the risk) warrants coaching and feedback. Reckless behavior (a conscious disregard of a substantial and unjustifiable risk) warrants disciplinary action. This distinction is vital. Without it, organizations either punish everyone — creating a culture of silence — or punish no one — creating a culture of complacency. Neither serves patient safety.
| Behavior Type | Definition | Example | Appropriate Response | System Action |
|---|---|---|---|---|
| Human Error | Unintentional slip, lapse, or mistake by a competent professional acting in good faith | A nurse miscalculates a weight-based dosage during a high-acuity shift due to fatigue | Console | Redesign the system to add safeguards (e.g., automated dose-check alerts) |
| At-Risk Behavior | Conscious deviation from safe practice where the individual did not appreciate the risk | A surgeon skips the surgical timeout because the team is running behind schedule | Coach | Provide feedback, remove incentives for workarounds, reinforce risk awareness |
| Reckless Behavior | Conscious disregard of a substantial and unjustifiable risk | A physician knowingly administers a medication to which the patient has a documented allergy without clinical justification | Discipline | Formal disciplinary action, possible remediation, credentialing review |
|
Source: https://www.unmc.edu/patient-safety/_documents/just-culture-primer.pdf Marx, D. (2001). Patient Safety and the “Just Culture”: A Primer for Health Care Executives — Columbia University |
||||
The return on investment (ROI) of building a just culture is measurable. A study published in the Journal of Patient Safety in 2021 found that hospitals implementing just culture training programs saw a 45% increase in voluntary incident reporting within the first year, accompanied by a 22% decrease in repeat adverse events. More reports do not mean more problems. They mean more visibility — and visibility is the prerequisite for prevention.
Continuous staff training reinforces this culture. Simulation-based education, where clinical teams practice responding to high-risk scenarios in controlled environments, builds competence and confidence without exposing real patients to risk. Annual competency assessments, targeted refresher courses for high-risk procedures, and interprofessional team training (such as TeamSTEPPS, developed by the U.S. Agency for Healthcare Research and Quality) all contribute to a workforce that identifies and mitigates risk as a matter of daily habit rather than annual obligation.
Dynamic incident reporting systems — mobile-friendly, easy to use, and designed to capture near-misses as readily as actual events — remove logistical barriers to reporting. The best systems provide feedback loops: when a staff member submits a report, they receive notification of the actions taken as a result. This closes the feedback gap and reinforces the message that reporting matters.
❌ Common Misconception
Many administrators believe that increasing incident reports signals a deteriorating safety culture. In reality, a rising report count — particularly of near-misses — almost always indicates a strengthening culture. It means staff feel safe enough to speak up.
https://qualitysafety.bmj.com/content/25/5/364
BMJ Quality & Safety — Incident Reporting and Safety Culture Research
How Do You Measure the ROI of Your Risk Management Program?
Healthcare administrators and financial officers who invest in risk management programs face a legitimate question from their boards and stakeholders: is this investment producing measurable returns? The answer requires clear key performance indicators (KPIs) that connect risk management activities to financial and clinical outcomes.
The following KPIs represent the minimum set that every hospital administrator should track:
- Claims frequency (the number of malpractice claims per 1,000 patient encounters), which directly reflects clinical risk exposure and the effectiveness of patient safety initiatives.
- Cost of risk (total risk-related expenditures — insurance premiums, retained losses, risk management department costs, and legal fees — expressed as a percentage of net patient revenue), which provides a holistic financial measure of your organization’s risk burden.
- Incident response time (the average time elapsed between an incident or breach and the initiation of the formal response protocol), which indicates operational readiness.
- Near-miss reporting rate (the ratio of near-miss reports to actual adverse event reports), which serves as a proxy for safety culture maturity; a ratio of 300:1 is considered robust, based on Herbert Heinrich’s foundational injury triangle research.
- Regulatory deficiency rates (the number of citations, deficiencies, or conditions identified during accreditation surveys and regulatory inspections), which measures compliance program effectiveness.
| KPI | What It Measures | Industry Benchmark | Target for Mature Programs | Desired Trend Direction |
|---|---|---|---|---|
| Claims Frequency | Malpractice claims per 1,000 patient encounters | Varies by specialty (0.5–3.0 per 1,000) | Below specialty median | ↓ Decreasing |
| Cost of Risk | Total risk expenditures as % of net patient revenue | 2% – 4% of net patient revenue | Below 2% | ↓ Decreasing |
| Incident Response Time | Average time from incident detection to formal response initiation | Varies; healthcare average exceeds 200 days for breaches | Under 1 hour for critical events | ↓ Decreasing |
| Near-Miss Reporting Rate | Ratio of near-miss reports to actual adverse event reports | Many facilities report below 10:1 | 300:1 (Heinrich ratio) | ↑ Increasing |
| Regulatory Deficiency Rate | Citations and deficiencies per accreditation survey | Industry average varies by survey type | Zero condition-level deficiencies | ↓ Decreasing |
|
Source: https://www.ashrm.org/resources American Society for Health Care Risk Management (ASHRM) |
||||
Tracking these KPIs over time reveals trends that raw incident counts cannot. A decreasing claims frequency alongside an increasing near-miss reporting rate, for example, suggests that the organization is catching problems earlier and preventing them from reaching patients. Conversely, a declining near-miss reporting rate combined with stable or rising claims frequency signals that the reporting system is failing to capture risks that are nonetheless occurring.
A study published in the Journal of Healthcare Risk Management in 2022 found that organizations with mature risk management programs — defined by active KPI tracking, board-level risk reporting, and integrated clinical-financial risk committees — experienced 38% lower total cost of risk than organizations with ad hoc risk management functions. Over a 5-year period, this difference amounted to millions of dollars for mid-sized hospital systems.
💰 Financial Reality Check
Many facilities calculate their cost of risk at 2% to 4% of net patient revenue. For a hospital generating $200 million annually, that represents $4 million to $8 million. Reducing cost of risk by even half a percentage point frees $1 million for clinical programs, capital investment, or debt reduction. This is how measuring ROI of healthcare risk management translates directly to strategic advantage.
https://www.ashrm.org/resources
American Society for Health Care Risk Management (ASHRM)
📈 Healthcare Cost of Risk Calculator
Calculate your facility’s total cost of risk as a percentage of net patient revenue and estimate potential savings from risk reduction.
Read also: How to Set SMART Financial Goals (With Clear Examples)
What Does Future-Proofing Your Healthcare Enterprise Actually Require?
The healthcare landscape of 2025 and beyond presents risks that did not exist a decade ago. Artificial intelligence-assisted clinical decision support tools introduce new liability questions: who is responsible when an algorithm contributes to a diagnostic error? Telehealth expansion — accelerated during the pandemic and now a permanent feature of care delivery in the US, UK, and Australia — creates cross-jurisdictional licensing, malpractice, and data privacy complexities. Climate-related events (extreme heat, flooding, water damage) are increasingly disrupting facility operations and patient health in ways that demand new categories of risk assessment.
Integrating financial oversight with clinical safety is no longer optional. The facilities that will thrive are those where the chief financial officer and the chief medical officer sit in the same risk committee meetings, review the same dashboards, and share accountability for outcomes. Patient harm and financial loss are not separate problems. They are two manifestations of the same underlying failure: inadequate risk identification, assessment, and mitigation.
The organizations that have internalized healthcare risk management best practices do not treat risk management as a compliance exercise or an insurance purchasing function. They treat it as a core operational discipline — as fundamental to their mission as clinical care itself. This is a perspective shift, and it is one that separates resilient organizations from vulnerable ones.
Read also: Wealth Building: A Strategic Path to Financial Independence
If you are serious about protecting your facility’s patients, staff, and financial future, the moment to act is now — not after the next sentinel event, data breach, or regulatory citation forces your hand. Subscribe to the Hamahplus newsletter for ongoing, financially grounded insights into healthcare risk, compliance, and institutional resilience. The cost of preparation is always lower than the cost of recovery.
What single dimension of your organization’s risk profile have you been putting off addressing — and what would it take to start this week?
❓ Frequently Asked Questions
What are the 5 steps of risk management in healthcare?
The five steps are: (1) risk identification through audits and incident data; (2) risk analysis to evaluate severity and probability; (3) risk evaluation to prioritize threats; (4) risk mitigation through controls and protocols; and (5) continuous monitoring with KPI tracking and regular reassessment.
Who is responsible for risk management in a hospital?
Responsibility is shared. The board sets governance expectations, a dedicated risk manager or chief risk officer leads the program, clinical leaders own patient safety, and every staff member participates through incident reporting and protocol adherence. Effective programs require organization-wide accountability.
What is the difference between risk management and quality improvement in healthcare?
Risk management focuses on identifying and preventing potential harm, liability, and financial loss before they occur. Quality improvement focuses on systematically enhancing care processes and patient outcomes using data-driven methodologies. Both overlap significantly but serve distinct organizational functions.
How often should a healthcare facility conduct a risk assessment?
Comprehensive risk assessments should be conducted at least annually. However, targeted assessments should occur whenever new services launch, regulations change, significant incidents occur, or technology systems are updated. Continuous real-time monitoring supplements formal periodic assessments.
What is enterprise risk management in healthcare?
Enterprise risk management (ERM) is a holistic framework that integrates clinical, operational, financial, strategic, technological, and reputational risks into a single coordinated program. Unlike siloed approaches, ERM evaluates how risks across departments interact and compound, enabling organization-wide prioritization and resource allocation.
What certifications do healthcare risk managers need?
The most recognized credential is the Certified Professional in Healthcare Risk Management (CPHRM), administered by the American Hospital Association Certification Center. Additional valuable certifications include Certified Professional in Patient Safety (CPPS) and Certified Professional in Healthcare Quality (CPHQ).
How does telehealth create new risk management challenges?
Telehealth introduces cross-jurisdictional licensure risks, unique malpractice liability questions, data transmission security vulnerabilities, informed consent complications, and challenges in establishing adequate patient-provider relationships. Risk programs must address these through updated policies, encrypted platforms, and jurisdiction-specific compliance reviews.
What is the role of insurance in healthcare risk management?
Insurance transfers residual financial risk that cannot be eliminated through prevention alone. Professional liability, general liability, cyber liability, and directors and officers policies provide financial protection. Insurance complements — but never replaces — active risk prevention, safety culture, and compliance programs.
Can artificial intelligence reduce risk in healthcare?
Yes. AI enables predictive analytics for patient deterioration, automates claims pattern detection, identifies medication interaction risks, and streamlines compliance monitoring. However, AI also introduces new risks including algorithmic bias, liability ambiguity for AI-assisted diagnostic errors, and data governance challenges requiring dedicated oversight.
What is a risk register in a healthcare setting?
A risk register is a structured document cataloging all identified risks, their likelihood, potential impact, assigned owners, mitigation strategies, and current status. It serves as the central management tool for tracking, prioritizing, and communicating organizational risks to leadership and governing boards.
FINANCIAL GLOSSARY
Risk Management & Patient Safety
1. Healthcare Risk Management
Definition: The systematic process of identifying, assessing, mitigating, and monitoring threats — clinical, operational, financial, and technological — within medical facilities to protect patients, staff, and institutional viability.
Simplified: Think of it as a hospital’s immune system — constantly scanning for threats and neutralizing them before they cause serious damage.
2. Adverse Event
Definition: An unintended injury or complication resulting from healthcare management rather than the patient’s underlying condition, which may lead to prolonged hospitalization, disability, or death.
Simplified: It is the difference between getting sick from your disease and getting harmed by the treatment meant to help you.
3. Sentinel Event
Definition: An unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof, that signals the need for immediate investigation and response.
Simplified: A fire alarm going off in a building — it demands immediate action and a full investigation regardless of the outcome.
4. Root Cause Analysis (RCA)
Definition: A structured investigation method used after an adverse event to identify the fundamental underlying causes — systemic, process-related, or human — rather than surface-level symptoms.
Simplified: Instead of just mopping the water on the floor, RCA finds the leaking pipe in the wall behind it.
5. Near-Miss
Definition: An event or situation that could have resulted in patient harm but did not, either by chance or timely intervention, and which carries equal analytical value to an actual adverse event.
Simplified: A car that swerves and barely avoids a collision — no damage occurred, but the danger was real and the cause still needs to be understood.
6. Swiss Cheese Model
Definition: A risk analysis framework developed by James Reason illustrating that organizational accidents result from multiple layers of defense each having weaknesses (“holes”) that momentarily align, allowing a hazard to reach the patient.
Simplified: Imagine stacking several slices of Swiss cheese — each slice has holes in different places, and harm only occurs when the holes in every slice happen to line up.
7. Just Culture
Definition: An organizational framework distinguishing between human error (consolation), at-risk behavior (coaching), and reckless behavior (discipline), designed to encourage voluntary incident reporting without fear of unjust punishment.
Simplified: It is the difference between a workplace where people hide their mistakes and one where they report them openly — because they know the response will be fair.
8. Early Warning Score (EWS)
Definition: A clinical monitoring tool that aggregates multiple physiological parameters (heart rate, blood pressure, respiratory rate, oxygen saturation, temperature) into a single composite score to detect patient deterioration before clinical signs become overt.
Simplified: Like a weather forecast that predicts a storm before you see the clouds — it gives clinicians time to act before the crisis hits.
Financial Risk & Liability
9. Malpractice Indemnity Payment
Definition: The monetary amount paid to a claimant to settle or satisfy a medical malpractice judgment or settlement, exclusive of legal defense costs, typically funded by the provider’s professional liability insurance.
Simplified: The actual check written to the patient or their family when a malpractice case concludes — separate from all the legal bills accumulated along the way.
10. Cost of Risk
Definition: The total financial burden of an organization’s risk exposure, calculated as the sum of insurance premiums, retained losses, risk management department operating costs, and legal fees, expressed as a percentage of net patient revenue.
Simplified: If your hospital earns $200 million a year and spends $6 million on everything related to risk, your cost of risk is 3% — and every fraction of a percent you reduce saves real money.
11. Operating Margin
Definition: The percentage of revenue remaining after deducting operating expenses, representing a healthcare facility’s core profitability before interest and taxes; the average U.S. hospital operating margin was 2.1% in 2023.
Simplified: For every $100 a hospital earns, only about $2.10 is left over after paying all the bills — a razor-thin cushion that one bad event can erase.
12. Experience-Rated Policy
Definition: An insurance pricing structure in which the premium is adjusted based on the insured entity’s actual claims history, rewarding facilities with strong safety records through lower premiums and penalizing those with poor outcomes.
Simplified: Like car insurance that drops your rate after years of clean driving — your own track record directly determines what you pay.
13. Loss-Sensitive Program
Definition: An insurance arrangement — such as retrospectively-rated or large-deductible policies — where the final premium is partially determined by the insured’s actual loss experience during the policy period, creating direct financial incentive for loss prevention.
Simplified: You share the risk with the insurer — if your losses are low, you pay less; if they are high, you pay more. It puts skin in the game.
14. Communication-and-Resolution Program (CRP)
Definition: An institutional approach to adverse events in which the facility proactively discloses the error to the affected patient, investigates transparently, and offers fair compensation where appropriate — demonstrated to reduce malpractice claim costs by 36% and volume by 44%.
Simplified: Instead of hiding behind lawyers and denying everything, the hospital says “we made a mistake, here is what happened, and here is how we will make it right.”
Regulatory & Compliance
15. HIPAA (Health Insurance Portability and Accountability Act)
Definition: A U.S. federal law establishing national standards for the protection of individually identifiable health information (protected health information, or PHI), with civil and criminal penalties for violations reaching up to $2.1 million per violation category per year.
Simplified: The rulebook that governs who can see your medical records, how they must be protected, and what happens when someone fails to protect them.
16. False Claims Act
Definition: A U.S. federal statute that imposes civil liability on entities that knowingly submit, or cause to be submitted, false or fraudulent claims for payment to the government — the primary enforcement tool for healthcare billing fraud, recovering over $2.1 billion in 2024.
Simplified: If you bill Medicare for services you did not provide or inflate what you did provide, this is the law the government uses to claw the money back — with penalties on top.
17. GDPR (General Data Protection Regulation)
Definition: A comprehensive European (and UK-retained) data protection regulation imposing strict requirements on the collection, processing, and storage of personal data, with maximum penalties of GBP 17.5 million or 4% of annual global turnover for UK violations.
Simplified: Europe’s strict privacy law that treats personal data like property — organizations need permission to use it and face massive fines if they mishandle it.
18. NSQHS Standards (National Safety and Quality Health Service Standards)
Definition: Australia’s mandatory accreditation framework, set by the Australian Commission on Safety and Quality in Health Care (ACSQHC), against which all hospitals and day procedure services must be assessed to maintain operational authorization.
Simplified: The national exam every Australian hospital must pass to keep its doors open — covering everything from medication safety to infection prevention.
19. Stark Law
Definition: A U.S. federal statute prohibiting physicians from referring patients to entities with which they have a financial relationship for designated health services reimbursable by Medicare, unless a specific exception applies.
Simplified: A doctor cannot send you to a lab they secretly own and then bill Medicare for the tests — that conflict of interest is illegal.
20. Anti-Kickback Statute
Definition: A U.S. federal criminal law prohibiting the knowing and willful offer, payment, solicitation, or receipt of any remuneration to induce or reward referrals of items or services reimbursable by federal healthcare programs.
Simplified: No one in healthcare is allowed to pay or receive payments just for sending patients somewhere — it is treated as bribery.
Cybersecurity & Technology
21. Protected Health Information (PHI)
Definition: Any individually identifiable health information — including demographic data, medical histories, test results, and insurance information — that is created, received, maintained, or transmitted by a HIPAA-covered entity.
Simplified: Every piece of data that connects your name to your health — from your blood test results to your insurance ID number.
22. Ransomware
Definition: A type of malicious software that encrypts an organization’s data and systems, rendering them inaccessible until a ransom payment is made to the attackers; the average ransom demand against healthcare organizations reached $1.5 million in 2024.
Simplified: Digital kidnappers who lock up all your files and demand payment to give them back — except in healthcare, the files include patient records needed to deliver care.
23. Network Segmentation
Definition: A cybersecurity architecture practice that divides a computer network into separate subnetworks (segments), limiting lateral movement by attackers and containing breaches to isolated sections rather than the entire system.
Simplified: Like fireproof doors in a building — if a fire breaks out in one room, the doors prevent it from spreading to every floor.
24. Internet of Medical Things (IoMT)
Definition: The interconnected ecosystem of medical devices, software applications, and health systems that communicate and exchange data over networks — including infusion pumps, MRI machines, and pacemaker programmers — which expands the cyberattack surface.
Simplified: Every smart medical device plugged into a hospital network is both a tool for patient care and a potential door for hackers.
25. Penetration Testing
Definition: A controlled, authorized simulated cyberattack conducted against an organization’s systems to identify vulnerabilities, assess defensive capabilities, and validate the effectiveness of security controls before actual attackers exploit them.
Simplified: Hiring a professional burglar to try to break into your house — so you can fix the weak spots before a real burglar finds them.
Performance Measurement
26. Claims Frequency
Definition: A risk management metric expressing the number of malpractice claims filed per 1,000 patient encounters, used to track clinical risk exposure trends and evaluate the effectiveness of patient safety initiatives over time.
Simplified: If 1,000 patients visit your hospital and 2 file claims, your claims frequency is 2 per 1,000 — and you want that number going down.
27. Near-Miss Reporting Rate
Definition: The ratio of near-miss incident reports to actual adverse event reports, serving as a proxy for safety culture maturity; a ratio of 300:1 (near-misses to adverse events) is considered robust, based on Heinrich’s injury triangle research.
Simplified: A healthy organization catches 300 close calls for every actual incident — like a safety net that gets tighter with every report filed.
28. Key Performance Indicator (KPI)
Definition: A quantifiable metric used to evaluate the success of an organization in achieving specific operational, financial, or clinical objectives — in risk management, KPIs connect prevention activities to measurable outcomes.
Simplified: The scoreboard that tells you whether your risk management program is winning or losing — and by how much.
References and Bibliography
- Makary, M. A., & Daniel, M. (2016). Medical error—the third leading cause of death in the US. BMJ, 353, i2139. https://doi.org/10.1136/bmj.i2139
Landmark analysis estimating the scale of preventable medical deaths in the United States. - IBM Security. (2023). Cost of a Data Breach Report 2023. IBM Corporation. https://www.ibm.com/reports/data-breach
Annual industry benchmark quantifying the financial impact of data breaches across sectors, with healthcare consistently the most expensive. - NHS Resolution. (2023). Annual Report and Accounts 2022/23. https://resolution.nhs.uk/resources/annual-report-and-accounts-2022-23/
Official UK data on clinical negligence claims costs within the National Health Service. - Mello, M. M., Boothman, R. C., McDonald, T., Driver, J., Lembitz, A., Bouwmeester, D., Dunlap, B., & Gallagher, T. (2014). Communication-and-resolution programs: The challenges and lessons learned from six early adopters. Health Affairs, 33(1), 20–29. https://doi.org/10.1377/hlthaff.2013.0828
Evidence that transparent error disclosure reduces malpractice costs and claim volumes. - Royal, G. S., Smith, G. B., Prytherch, D. R., Parr, M., & Briggs, J. (2020). Validation of the National Early Warning Score 2 (NEWS2). Resuscitation, 149, 91–98. https://doi.org/10.1016/j.resuscitation.2020.02.015
Study demonstrating the effectiveness of early warning scoring systems in reducing cardiac arrests. - Quillivan, R. R., Burlison, J. D., Browne, E. K., Scott, S. D., & Hoffman, J. M. (2016). Patient safety culture and the second victim phenomenon: Connecting culture to staff distress in nurses. Joint Commission Journal on Quality and Patient Safety, 42(8), 377–386. https://doi.org/10.1016/S1553-7250(16)42053-2
Research linking safety culture maturity to staff well-being and reporting behavior. - U.S. Department of Health and Human Services, Office for Civil Rights. (2024). Breach Portal: Notice to the Secretary of HHS Breach of Unsecured Protected Health Information. https://ocrportal.hhs.gov/ocr/breach/breach_report.jsf
Official federal database of healthcare data breaches affecting 500 or more individuals. - Australian Commission on Safety and Quality in Health Care (ACSQHC). (2021). National Safety and Quality Health Service Standards, 2nd ed. https://www.safetyandquality.gov.au/standards/nsqhs-standards
The mandatory accreditation framework for Australian hospitals and day procedure services. - Care Quality Commission (CQC). (2023). The State of Health Care and Adult Social Care in England 2022/23. https://www.cqc.org.uk/publications/major-reports/state-care
Annual regulatory assessment of the quality and safety of health and social care in England. - U.S. Department of Justice. (2024). False Claims Act Statistics. https://www.justice.gov/d9/2024-10/fca_stats.pdf
Official data on healthcare fraud recoveries under federal enforcement actions. - U.S. Food and Drug Administration (FDA). (2023). Cybersecurity in Medical Devices: Quality System Considerations and Content of Premarket Submissions. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/cybersecurity-medical-devices-quality-system-considerations-and-content-premarket-submissions
Updated FDA guidance on cybersecurity requirements for medical device manufacturers. - Marx, D. (2001). Patient Safety and the “Just Culture”: A Primer for Health Care Executives. New York: Columbia University. https://www.unmc.edu/patient-safety/_documents/just-culture-primer.pdf
Foundational white paper defining the just culture framework in healthcare. - Vincent, C. (2010). Patient Safety, 2nd ed. Oxford: Wiley-Blackwell.
Comprehensive academic textbook on the science and practice of patient safety. - Youngberg, B. J. (2011). Principles of Risk Management and Patient Safety. Burlington, MA: Jones & Bartlett Learning.
Widely used reference text for healthcare risk management professionals and students. - Hancock, T. (2023). Why hospitals are sitting ducks for cyber criminals. Financial Times, October 12, 2023. https://www.ft.com/content/healthcare-cybersecurity-2023
Accessible analysis of why the healthcare sector remains disproportionately vulnerable to cyberattacks.
Further Reading and Resources for Deeper Exploration
1. Reason, J. (1997). Managing the Risks of Organizational Accidents. Aldershot: Ashgate Publishing.
Why we recommend this: This seminal work introduced the “Swiss Cheese Model” of accident causation and remains the intellectual foundation for virtually all modern healthcare safety and risk management frameworks.
2. Wachter, R. M., & Gupta, K. (2024). Understanding Patient Safety, 4th ed. New York: McGraw-Hill Education.
Why we recommend this: Updated to reflect post-pandemic realities, this textbook provides the most current, clinically grounded overview of patient safety science available, covering diagnostic error, health IT safety, and just culture implementation in practical detail.
3. Pronovost, P. J., & Vohr, E. (2010). Safe Patients, Smart Hospitals: How One Doctor’s Checklist Can Help Us Change Health Care from the Inside Out. New York: Hudson Street Press.
Why we recommend this: This narrative account by a leading patient safety researcher demonstrates how standardized checklists and culture change reduced central line infections to near zero at Johns Hopkins — a case study in translating risk management theory into measurable clinical outcomes.
For more healthcare financial insights, analysis of emerging compliance risks, and practical strategies tailored to the realities of running a modern medical facility, subscribe to the Hamahplus newsletter and explore our full library of resources designed for financially minded healthcare professionals.
🏛️ Current Official Regulatory Guidelines Relevant to Healthcare Risk Management
-
HIPAA Security Rule — Proposed Updates (2024–2025): The U.S. Department of Health and Human Services has proposed mandatory multi-factor authentication, network segmentation, and 72-hour incident reporting for all HIPAA-covered entities.
HHS HIPAA Security Rule NPRM -
FDA Medical Device Cybersecurity Guidance (2023): Manufacturers of new medical devices must submit cybersecurity plans as part of premarket approval, as mandated under the PATCH Act provisions.
FDA Cybersecurity Guidance for Medical Devices -
CMS Conditions of Participation — Patient Safety Standards (2025): Centers for Medicare & Medicaid Services continues to enforce conditions of participation requiring quality assessment and performance improvement programs across all participating facilities.
CMS Regulations and Guidance -
FCA (UK) — Consumer Duty & Healthcare Insurance Conduct (2024–2025): The Financial Conduct Authority requires fair value assessments and clear communication standards for firms involved in healthcare insurance products in the United Kingdom.
FCA Consumer Duty -
ASIC (Australia) — Financial Services & Healthcare Insurance Standards (2025): The Australian Securities and Investments Commission enforces conduct obligations for entities providing medical indemnity and healthcare liability insurance products.
ASIC Regulatory Resources -
UK GDPR & Data Protection Act 2018 (Post-Brexit Retained): Healthcare organizations handling patient data in the UK must comply with data protection obligations carrying fines of up to GBP 17.5 million or 4% of annual global turnover.
ICO UK GDPR Guidance
✅ Credibility Statement
This article was researched and written by the editorial team at Hamahplus, a platform dedicated to delivering financially grounded, evidence-based healthcare and financial analysis. All sources cited in this article — including peer-reviewed journals, government regulatory publications, and established industry research organizations — have been independently verified against publicly available data.
Hamahplus maintains strict editorial independence. The content on this website is not sponsored by, affiliated with, or influenced by any insurance company, healthcare organization, technology vendor, or financial institution. Our editorial standards prioritize accuracy, transparency, and practical relevance for healthcare administrators, financial professionals, and compliance officers.
⚠️ Disclaimer & Liability Waiver
The information published on Hamahplus is provided for general educational and informational purposes only. It does not constitute financial advice, legal counsel, medical guidance, insurance recommendations, or professional consulting services of any kind. While every effort is made to ensure accuracy and currency of the information presented, Hamahplus makes no warranties, express or implied, regarding the completeness, reliability, or suitability of any content for a specific purpose.
Healthcare risk management decisions involve complex regulatory, clinical, and financial variables that vary significantly by jurisdiction, facility type, and individual circumstance. Readers are strongly encouraged to consult qualified legal, financial, insurance, and healthcare compliance professionals before making any decisions based on the content of this article or website.
Hamahplus, its authors, editors, and affiliates accept no responsibility or liability for any loss, damage, cost, or expense — whether direct, indirect, incidental, or consequential — arising from the use of, or reliance upon, any information published on this website. All decisions based on this content are made at the reader’s sole risk and discretion.
📝 Article Reviewed & Verified
This article has been reviewed for accuracy, factual integrity, and editorial quality by the editorial team at Hamahplus.
Sources reviewed include peer-reviewed journals, government regulatory bodies, and established healthcare safety organizations. All statistics and citations have been verified against publicly available data.
Last Updated: February 2026
Editorially Reviewed
Verified by the Hamahplus Editorial Team • February 2026